

The Sweden study on psych meds correlation to increased ALS diagnosis

https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2834877
This study just published this week states that the use of anxiolytic, hypnotic, and antidepressant medications could be associated to higher incidence of ALS, a devastating neuron disorder that is fatal.
Soundbites:
They do not specifically list what meds in each category were evaluated.
The study period was 2015-2023
The patient with ALS had to have had 1-2 prescriptions of one of the above medications prior to ALS diagnosis to be considered part of the study group
The overwhelming majority of ALS diagnosis was among men over age 65
There were 1,057 study participants and 5,021 population control participants.
Study conclusions showed that antidepressants carried the highest risk for possible future ALS diagnosis.
I like digging into these kinds of studies because I am specialized in psychiatry. We obviously do not want to give medications that have a risk of a life altering condition such as ALS. My biggest concern here was what medications were they using in Sweden in the study criteria that showed potential for ALS diagnosis increase. The study does not list them. BUT. I was able to source the most commonly used medications in Sweden through AI search. Here is what I found:
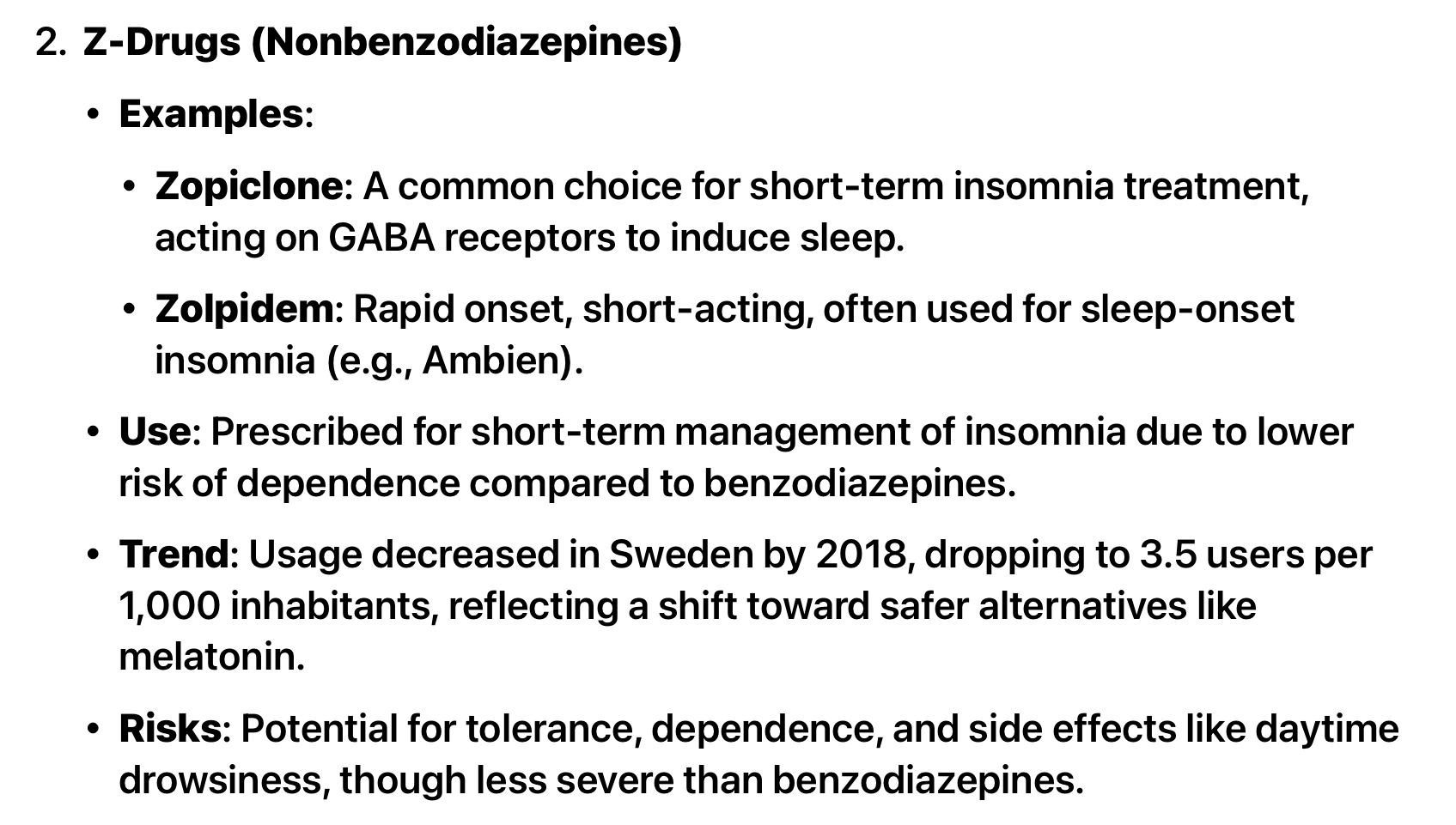
First off, they use the same antidepressants in Sweden that we typically see used here in the United States. They also use the same z-drug sleep meds such as Ambien and Lunesta. But the Benzodiazepines they use in Sweden are much different. They trend in using Oxazepam and Valium, whereas here in the US, we do not use those in outpatient care.
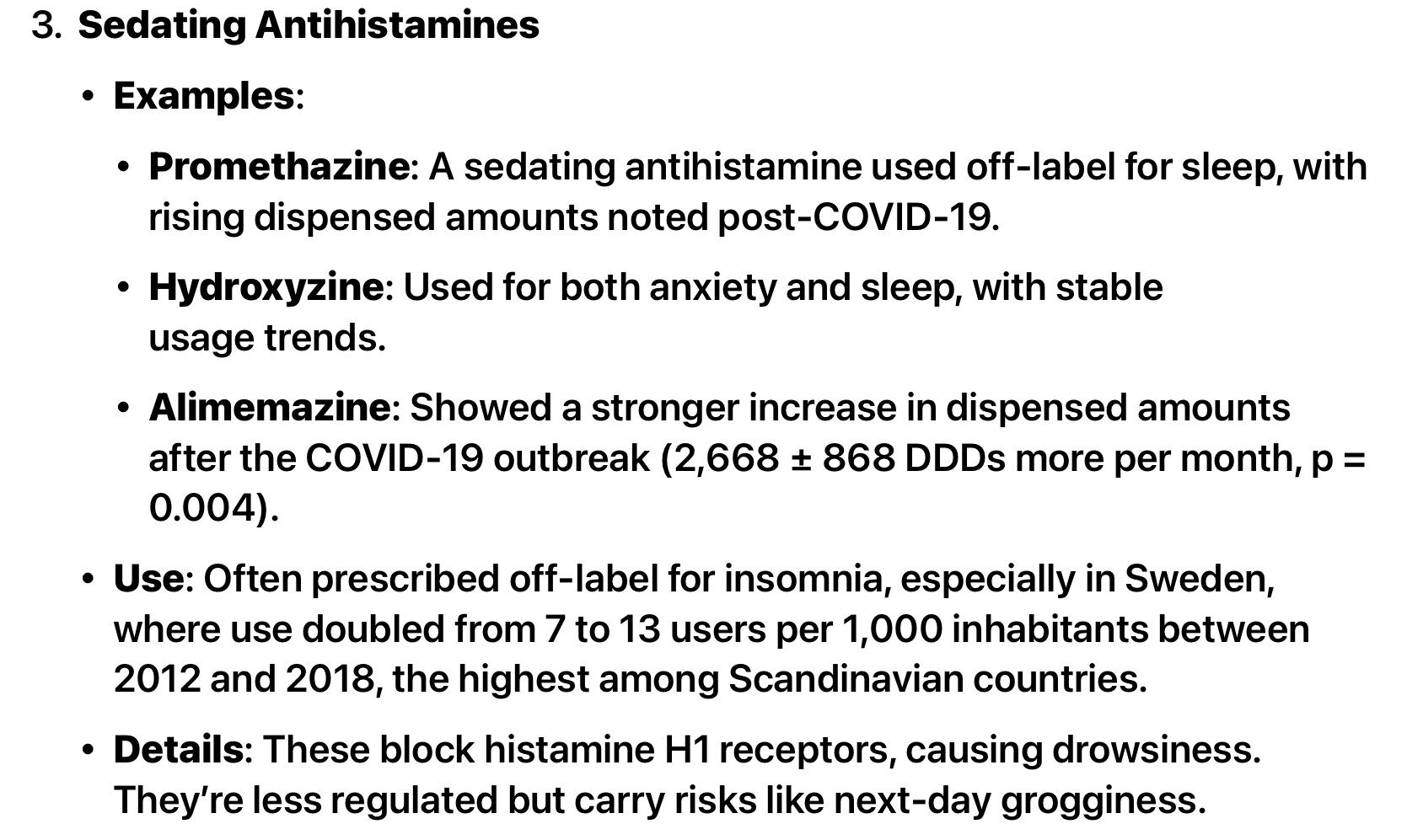
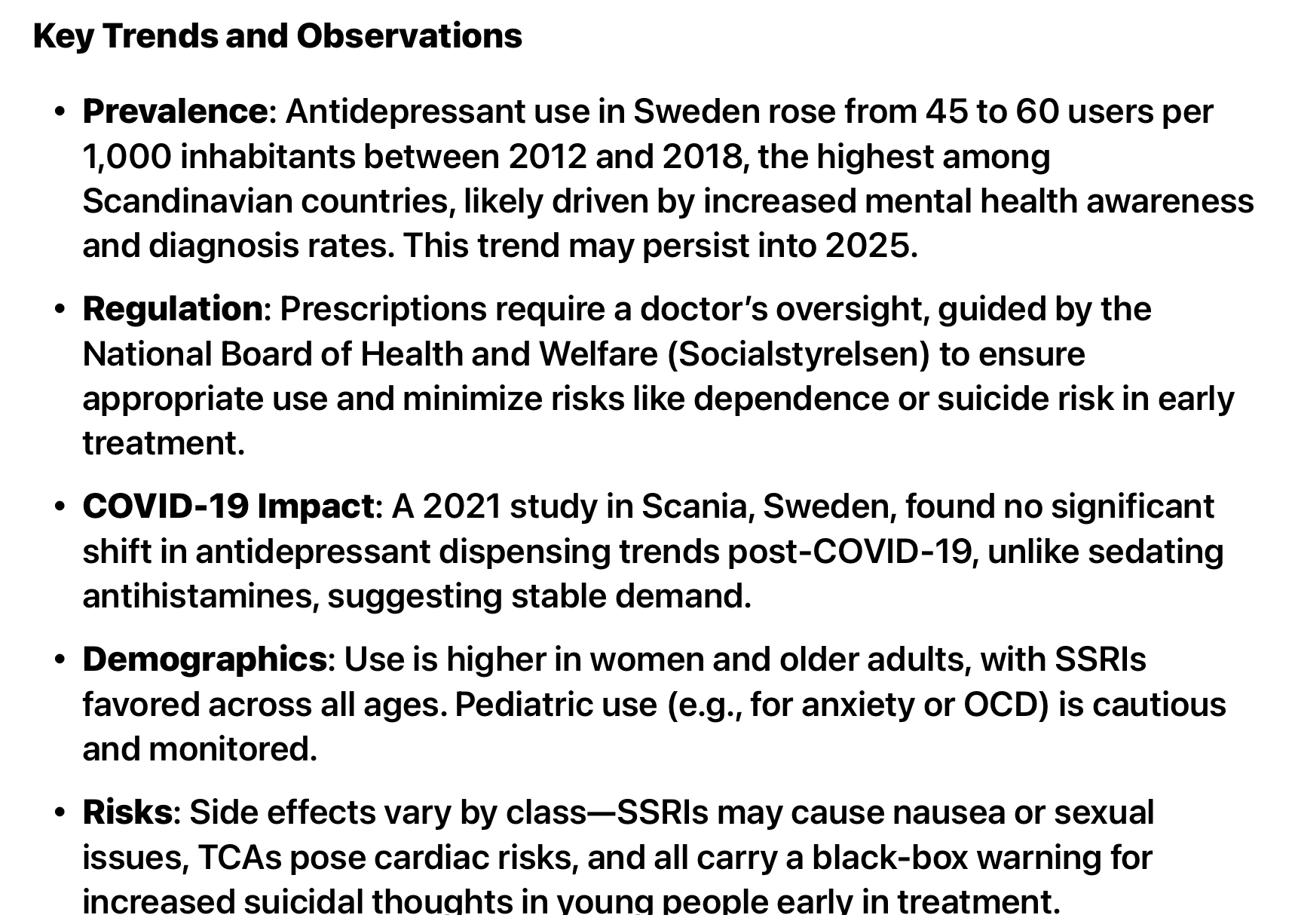
The findings from the Sweden drug search note that SSRI prescribing went through the roof, while z-drug and benzodiazepine prescribing had dropped significantly by 2018. This study ran from 2015-2023. The use of z-drugs and benzodiazepines had already dropped off significantly. But look at what the trend was on SSRI/SNRI medications and antihistamines like promethazine and Hydroxyzine. They were much higher and continued to trend higher. One of the limitations of this study is it never says if a person was given 10 tablets of a benzo or 14 days of a z-drug historically, taken for a 1 time duration only, it lumps all of the meds into one category including those who had a longer duration prescription. It also does not account for dosage on ANY class of meds.
I would like to see a study that lists WHAT the actual drug was the person took, how long they took it for, and the dose. Rather than lumping an entire class into the risk, we need to look at the actual DRUG that was potentially associated with the elevated risk.
The reason I want to see that data? We cannot generalize that because drug A caused a problem, then drug B will cause the same problem. There are several meds I flat out don’t prescribe solely from a risk/benefit profile. But studies like these are what people will cling onto to say no, I am never prescribing that drug class of meds, because it was in a generalized study. These are also the kinds of studies that insurance companies will use to deny a patient a medication sent by a provider.
We are all for safety. If there is a dirty rotten med among the bunch let’s name them and get rid of them. But we have to stop generalizing just a drug class in these kinds of studies. And they need to account for why they have had sky rocketing SSRI prescribing when that drug class has a black box warning (see the screen shot above).
I am not defending or berating any of the meds used in Sweden, but I would love to have more definitive studies done and less generalization. I cannot attribute ALS risk to a person who was given a one time dose of Valium prior to an MRI and a one time dose of Ambien prior to a sleep study without showing me what med was given for what duration prior to ALS diagnosis, but never took any other psych drug prior to ALS diagnosis. Because the criteria for this study was a patient received 1-2 “prescriptions” of any of those 3 category meds prior to ALS diagnosis. A single pill given 2 times would fit that criteria. I suspect they have that data, but it doesn’t fit the narrative, so they opted to generalize.
If they have accurately correlated certain drugs to ALS, that needs to be studied much further, possibly with protocols targeting certain drugs. ALS is a death sentence. You do not go quietly into the night, however. You deteriorate, and all those around feel your pain. It is worse than Dementia and Alzheimers. My personal opinion would be to avoid any of these types of drugs. We do not have a good enough understanding of the brain and the physiology of people. There are so many holistic treatments for depression. Unfortunately, they require exercise of the body and the brain and most people, as we learned during the fake pandemic, are just too lazy to take care of themselves. We work with several neuro stimulation devices. These devices are treating stroke, Parkinsons and Alzheimers. Sometimes with amazing results. Talk to the engineers about ALS and they will tell you they are not even trying. Sadly, the drug industry as we all learned during the fake pandemic only cares about profit. They will try and bury this study and be sure funding is NOT available for further studies.
Great point, Jennifer!
Drug A may not cause known issues.
But when used in combination with Drug B or C, may have unforseen consequences.
Raw data is essential.