

Part 2: The autoimmune hepatitis story continues……..

Around the same time that local news networks were releasing information about “possible adenovirus caused autoimmune hepatitis in children”, this journal of Hepatology article came out (April 22nd, 2022).
https://www.journal-of-hepatology.eu/article/S0168-8278(22)00234-3/fulltext
“Autoimmune hepatitis episodes have been described following SARS-CoV-2 infection and vaccination but their pathophysiology remains unclear. Here, we report the case of a 52-year-old male, presenting with two cases of acute hepatitis, each occurring 2-3 weeks after BNT162b2 mRNA vaccination “ (Pfizer vaccine). So this gentleman had acute hepatitis TWICE. Both times were 2-3 weeks after his Pfizer vaccine. Coincidence??? Probably not.
The study goes on to discuss “Liver inflammation is observed during SARS-CoV-2 infection as well as in individuals after vaccination and shares some typical features with autoimmune liver disease. In this report, we show that highly activated T cells accumulate and are evenly distributed in the different areas of the liver in a patient with liver inflammation following SARS-CoV-2 vaccination. Moreover, within these liver infiltrating T cells, we observed an enrichment of T cells that are reactive to SARS-CoV-2, suggesting that these vaccine-induced cells can contribute to the liver inflammation in this context.” The study goes further and states “Liver injury was observed after both mRNA and vector-based vaccines, while time from vaccine administration to symptom onset ranged between 4 days after the first dose to 6 weeks after the second dose. One patient was re-exposed to the vaccine which led to a worsening of liver injury. It remains unclear whether the reported association of autoimmune hepatitis with vaccination is coincidental, might reflect transient drug-induced liver injury, or could involve unique SARS-CoV-2-induced antigen-specific immune activation. However, the fact that autoimmune hepatitis-like conditions also occurred after SARS-CoV-2 infection suggests that the latter could be a driving factor for the sporadic cases.” (Saving them a convenient OUT here to blame the virus on the cause, not the vaccine. Despite this case study being in a covid vaccinated patient with hepatitis post BOTH COVID VACCINES).
The course of illness for this patient in this paper went like this: The 52-year-old male patient with no remarkable medical history other than hypothyroidism under long-term substitution therapy with levothyroxine and normal historic liver function tests (LFT) developed progressive nausea, fatigue, loss of appetite and pruritus with symptoms starting approximately 10 days after the first (prime) dose of the Pfizer BNT162b2 mRNA vaccine. He subsequently developed jaundice and presented at his primary care physician with LFT indicative of acute hepatitis. Liver enzymes were elevated, so was bilirubin. The patient was admitted to a primary care center 25 days post first vaccination. Viral hepatitis A, B, C and E as well as cytomegalovirus- and Epstein-Barr virus-infections were ALL NEGATIVE by serology and/or PCR testing. There was also no significant alcohol consumption and autoimmune serology remained inconclusive with borderline AMA-M2 reactivity. The patient recovered rapidly and was discharged with decreasing LFTs after three days with a diagnosis of a toxic hepatitis. Over the next two weeks, liver enzymes declined further, with normalization of AST and ALT and the patient received his second (boost) dose of the BNT162b2 mRNA vaccine 41 days after the first vaccination. 20 days post boost vaccination, the patient re-experienced nausea and fatigue. Lab testing revealed a relapse of acute mixed hepatitis 26 days post 2nd vaccine. We performed a liver biopsy that histologically showed findings are compatible with a probable autoimmune hepatitis. Over the next weeks liver enzymes declined before a HEPATITIS RELAPSE occurred 39 days after initial recurrent symptoms they went to the hospital, now 66 days post 2nd vaccine. The patient’s liver enzymes subsequently normalized after 8 weeks of additional treatment.
Findings include: The early increase in liver enzyme values after first and second dose of BNT162b2 and the observation that CD8 T cells including spike-specific CD8+ T cells dominate the immune infiltrate also fits to recent observations that demonstrate an early mobilization of spike-specific CD8 T cells already after the first dose of the vaccine. Also, Importantly, autoimmune hepatitis is a condition that requires lifelong immunosuppressive therapy in many affected patients. So much like myocarditis, this is not just an easy to recover self limiting disease. This becomes a chronic life long disease that affects the patient for the rest of their life. Some end up requiring a liver transplant. Life long following with a hepatologist to monitor liver function.
This study is important for many reasons. First off, the mainstream media has worked VERY HARD to claim the new cases of pediatric hepatitis are 100% definitely not vaccine related. However, the onset of these cases started in the fall of 2021. When were clinical trials and initial vaccinations started for kids and teenagers? Oh yeah, back in 2021. Last fall we were vaccinating pediatric patients.
Also remember, if we go back into the “way back machine” and you look at the slides from the Pfizer data post on the April 11th post I shared…….what was the ONE MAIN ORGAN where the covid vaccine went post vaccine? THE LIVER. Here is that table for review again:
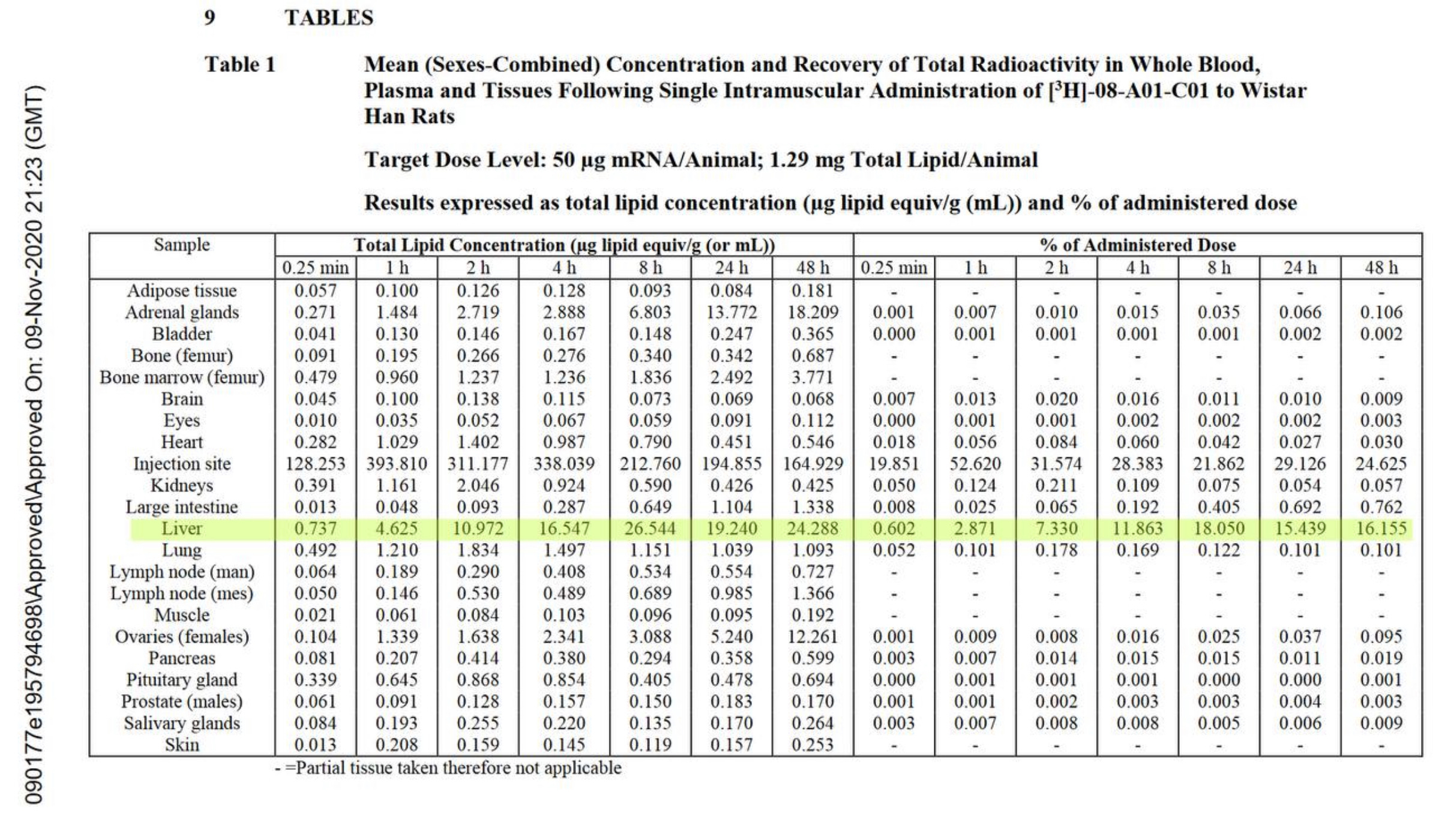
So we knew that at least 16% of the vaccine was going TO the liver. That is from Pfizer’s own delayed data release. Coincidentally, in October 2021, we start seeing “autoimmune hepatitis” starting in kids. But it is definitely NOT the vaccine causing these cases. Uh huh. Right. Per the NHS guidelines in Europe, where the majority of pediatric hepatitis cases are occurring, the NHS began rolling out the Pfizer Covid-19 injection to five million 5 to 11-year-old children in the UK at the beginning of April 2022. It had previously been administering it to young children deemed vulnerable since the end of 2021. Is it just a coincidence that a mere few weeks later an extremely concerning number of children are suffering hepatitis of unknown cause? A form of hepatitis so severe that children are requiring liver transplants, and losing their lives. They can blame it solely on a rogue adenovirus all they want to. Reduced immunity from masks and lockdowns. Scream from the rooftops that it isn’t the covid vaccine. The studies so far do not support their hypothesis. It sounds like one huge diversion and distraction event. Lets talk about vaccinated moms breastfeeding babies who now have autoimmune hepatitis. Lets talk about recently vaccinated people shedding the virus for 30 days being around kids who now have autoimmune hepatitis. Lets talk about the kids who were covid vaccinated. Lets stop ignoring the elephant in the room. We do not know the cause entirely yet. But we have plenty of puzzle pieces that say you cannot DEFINITIVELY SAY IT WAS NOT THE COVID VACCINE.